BioAcyl Corp |
|
Mallat, Z., & Binder, C. J. (2022). The why and how of adaptive immune responses in ischemic cardiovascular disease. Nature cardiovascular research, 1(5), 431–444. Added by: Dr. Enrique Feoli (07/04/2024, 18:10) Last edited by: Dr. Enrique Feoli (08/04/2024, 10:21) |
| Resource type: Journal Article Published DOI: 10.1038/s44161-022-00049-1 ID no. (ISBN etc.): 2731-0590 BibTeX citation key: Mallat2022 View all bibliographic details |
Categories: BioAcyl Corp Subcategories: Atherosclerosis/Inaflammation Keywords: , Creators: Binder, Mallat Collection: Nature cardiovascular research |
Views: 5/89
|
| Abstract |
|
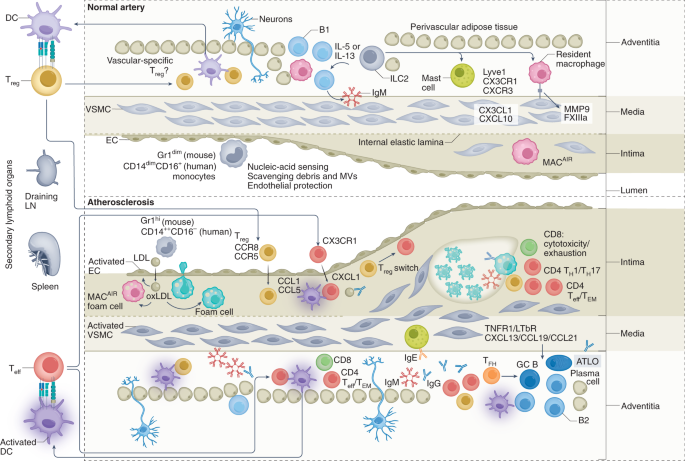
Atherosclerotic cardiovascular disease is a major cause of disability and death worldwide. Most therapeutic approaches target traditional risk factors but ignore the fundamental role of the immune system. This is a huge unmet need. Recent evidence indicates that reducing inflammation may limit cardiovascular events. However, the concomitant increase in the risk of life-threatening infections is a major drawback. In this context, targeting adaptive immunity could constitute a highly effective and safer approach. In this Review, we address the why and how of the immuno-cardiovascular unit, in health and in atherosclerotic disease. We review and discuss fundamental mechanisms that ensure immune tolerance to cardiovascular tissue, and examine how their disruption promotes disease progression. We identify promising strategies to manipulate the adaptive immune system for patient benefit, including novel biologics and RNA-based vaccination strategies. Finally, we advocate for establishing a molecular classification of atherosclerosis as an important milestone in our quest to radically change the understanding and treatment of atherosclerotic disease. VALT is present in normal, healthy arteries and comprises a variety of immune cells that serve essential roles in immune surveillance and vascular homeostasis. Crawling monocytes (Gr1dim in mice, CD14dimCD16+ in humans) sense nucleic acids, and those released after EC damage scavenge debris and microvesicles (MVs) and ensure EC protection. Intimal macrophages (MACAIR) accumulate at sites of intimal thickening (upper right, normal artery) and are the first myeloid cells that scavenge oxLDL in the initial stages of atherosclerosis (middle left, atherosclerotic plaque). This further drives vascular inflammation and leads to the recruitment of inflammatory monocytes (Gr1hi in mice; CD14++CD16− in humans) that give rise to a variety of macrophage subsets. Adventitial macrophages, particularly Lyve1+ macrophages (upper right, normal artery), regulate arterial stiffness, in part through the production of MMP9 and FXIIIA. Their specific contribution to atherosclerosis is currently unknown. The adventitia and perivascular adipose tissue form a permissive niche for the accumulation of atheroprotective ILC2 and innate-like B cells, organized in FALCs (upper middle, normal artery). ILC2-derived type 2 cytokines (for example, IL-5 and IL-13) promote B1 cell activation and the production of natural IgM antibodies, and contribute to an anti-inflammatory macrophage phenotype. Most DCs and T cells of normal arteries are found in the adventitia. T cells of normal arteries are likely to be enriched for a regulatory phenotype146, instructed by DCs presenting vascular-associated antigens (in draining lymphoid organs) and maintaining peripheral tolerance. The inflammatory milieu of developing lesions promotes DC maturation, which favors the generation of TH cells, Teff cells and TEM cells (mostly in draining lymphoid organs) and their recruitment into both the intima and adventitia of atherosclerotic arteries (bottom left). Sustained stimulation of autoreactive Treg cells may downregulate Foxp3, promoting their conversion into TH1 cells and Teff cells. Some of the Treg cells and Teff cells acquire a resident memory phenotype. TH1 cells, Teff cells and TEM cells predominate in advanced lesions (bottom right), and activated cytotoxic CD8+ T cells may acquire an exhausted phenotype. GC activation in secondary lymphoid organs leads to the production of affinity-matured class-switched (IgG, IgE) antibodies, which accumulate in lesions. Medial VSMCs of advanced lesions produce CXCL13 and CCL21 and may adopt features of lymphoid tissue organizer-like cells, leading to ATLO formation (bottom right). ATLOs are conducive to the generation of Treg cells, which serve a counter-regulatory, atheroprotective role. The diseased adventitia also establishes neuro–immune vascular interactions, which affect lesion progression. Added by: Dr. Enrique Feoli Last edited by: Dr. Enrique Feoli |
| Notes |
|
Ischemic InjuryThe heart and its adjacent pericardial and adipose tissue harbor several types of immune cells. a, At steady state, conventional DCs (cDCs), particularly cDC1, home to draining LNs and instruct the generation of tissue-specific (for example, myosin heavy chain-α) Treg cells146, which establish peripheral tolerance. Heart-derived HGF binds to DCs and induces an immune-regulatory phenotype. HGF also promotes chemokine production (for example, of CCL5) by c-MET-expressing T cells, which drives CCR5-dependent recruitment and cardiac Treg cell accumulation. Treg cell immunosuppressive function is further promoted through a local (cardiac) paracrine/autocrine adenosinergic loop, involving CD39/CD73 and adenosine A2A receptor (A2AR), or by engaging ST2 signaling with heart-derived IL-33. Pericardial innate lymphoid cells type 2 (ILC2)-derived IL-5 and IL-13 activate innate-like B cells to produce natural IgM antibodies and anti-inflammatory IL-10, which contribute to an anti-inflammatory and reparative macrophage phenotype. b, During ischemic injury, DCs acquire an inflammatory phenotype that provides instructions for the development of TH cells, Teff cells and TEM cells, as well as CD8+ cytotoxic T cells. Enhanced production of GM-CSF by pericardial innate-like B cells further promotes DC activation and the generation of TH cells and Teff cells. These T cells upregulate CX3CR1 and CXCR3, and their recruitment into the ischemic heart is facilitated by heart-derived CX3CL1 and CXCL10. GC reactions develop in the spleen and draining LNs, leading to the production of (heart-specific) autoantibodies, with potential detrimental consequences. Splenic MZ B cells are activated by the release of DAMPs, including in the form of mitochondria-containing microvesicles, which activate Toll-like receptors (TLRs), leading to CCL7 production. The latter promotes inflammatory monocyte mobilization from the bone marrow, enhancing the accumulation of inflammatory macrophages within the ischemic myocardium. In most cases, the ischemic heart is able to maintain the presence of a sufficient number of Treg cells to prevent the occurrence of overt full-blown cardiac autoimmunity. Added by: Dr. Enrique Feoli Last edited by: Dr. Enrique Feoli |
.")