BioAcyl Corp |
|
Steinman, J. B., Lum, F. M., Ho, P. P.-K., Kaminski, N., & Steinman, L. (2020). Reduced development of COVID-19 in children reveals molecular checkpoints gating pathogenesis illuminating potential therapeutics. Proc. Natl. Acad. Sci. U.S.A. 117(40), 24620–24626. Added by: Dr. Enrique Feoli (08/10/2020, 15:10) Last edited by: Dr. Enrique Feoli (20/04/2021, 12:03) |
| Resource type: Journal Article DOI: 10.1073/pnas.2012358117 ID no. (ISBN etc.): 0027-8424 BibTeX citation key: Steinman2020 View all bibliographic details |
Categories: BioAcyl Corp Subcategories: COVID-19 Creators: Ho, Kaminski, Lum, Steinman, Steinman Collection: Proc. Natl. Acad. Sci. U.S.A. |
Views: 2/267
|
| Abstract |
|
The reduced development of COVID-19 for children compared to adults provides some tantalizing clues on the pathogenesis and transmissibility of this pandemic virus. First, ACE2, the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) receptor, is reduced in the respiratory tract in children. Second, coronavirus associated with common colds in children may offer some protection, due to cross-reactive humoral immunity and T cell immunity between common coronaviruses and SARS-CoV-2. Third, T helper 2 immune responses are protective in children. Fourth, surprisingly, eosinophilia, associated with T helper 2, may be protective. Fifth, children generally produce lower levels of inflammatory cytokines. Finally, the influence of the downturn in the global economy, the impact of living in quarters among families who are the most at risk, and factors including the openings of some schools, are considered. Those most disadvantaged socioeconomically may suffer disproportionately with COVID-19.
|
| Notes |
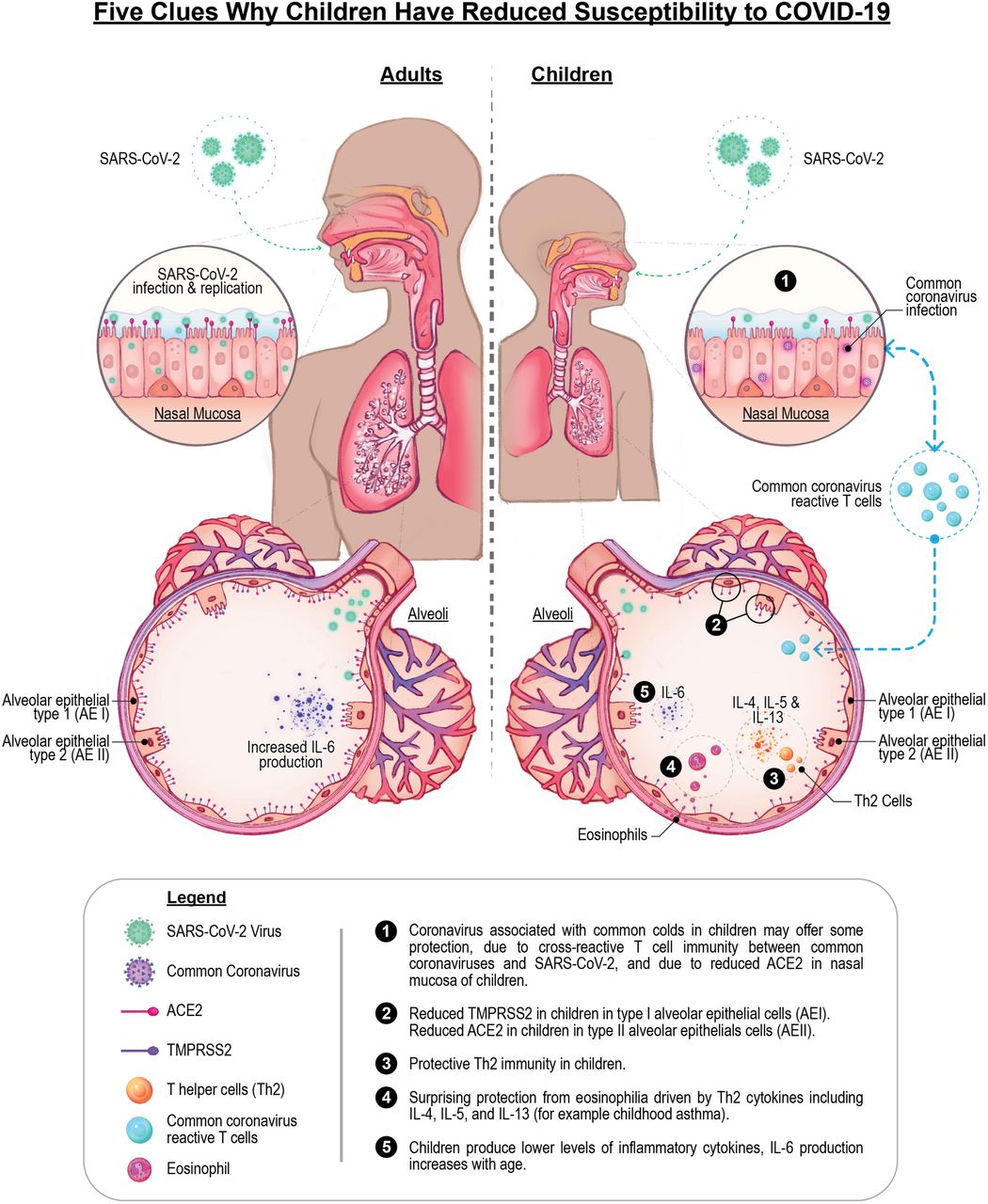
(1) Coronavirus associated with common colds in children may offer some protection due to cross-reactive T cell immunity and cross-reactive antibody immunity between common coronaviruses and SARS-CoV-2, and due to reduced ACE2 in nasal mucosa of children. (2) Reduced TMPRSS2 in children in type I alveolar cells (AEI). Reduced ACE2 in children in type II alveolar cells (AEII). (3) Protective Th2 immunity in children. (4) Surprising protection from eosinophilia driven by Th2 cytokines including IL-4, IL-5 and IL-13 (for example childhood asthma). (5) Children produce lower levels of inflammatory cytokines, IL-6 production increases with age. Th2 may be associated with iBALT
Viral Interference.Often, children are infected by more than one viral agent (21, 22). Viral interference is a well-known phenomenon where one virus interferes with the replication of a second virus (23). There is some evidence for coinfections in COVID-19 patients, including coinfection with other coronaviruses (24, 25). Kim et al. (24) reported on both hospitalized and nonhospitalized cases from Northern California, including children. They found more than 20% were positive for a second viral infection, including infection with other coronaviruses. In contrast, Nowak et al. (25) reported concurrent viral infection in only 3% of 1,204 SARS-CoV-2−positive patients from the New York metropolitan area who were also tested with a respiratory virus panel or a test for influenza and respiratory syncytial virus (RSV). In comparison, of 7,418 patients who tested negative for SARS- CoV-2, 845 were tested with the same multiplex panels, and 13% were positive for at least one non-SARS-CoV-2 respiratory viral pathogen (25). The increase in at least one non-SARS-CoV-2 viral pathogen in those who tested negative for SARS-CoV-2 may be due, in part, to viral interference. An intriguing potential mechanism of resistance in children is that common coronaviruses associated with mild illnesses like colds and more severe illness like croup and bronchiolitis are associated with decreased expression of ACE2. For example, human coronavirus (HCoV) NL63, associated with common colds and croup, induces a down-regulation of ACE2 (26). A reduction in the viral receptor for SARS-CoV-2 therefore might help explain why children who carry such viruses in their nose and upper portions of their respiratory tracts are hospitalized less frequently than adults. The first site of encounter in the respiratory tract for the SARS-CoV-2 is in the nose. Investigators studying a cohort of 305 patients aged 4 y to 60 y found that “older children (10 y to 17 y old; n = 185), young adults (18 y to 24 y old; n = 46), and adults (≥25 y old; n = 29) all had higher expression of ACE2 in the nasal epithelium compared with younger children (4 y to 9 y old; n = 45)” (27). Despite diminished expression of ACE2 and/or TMPRSS2 in children, “symptomatic infants have higher nasopharyngeal SARS-CoV-2 viral loads at presentation but develop less severe disease than older children and adolescents” (28). Moreover, children less than 5 y old “with mild to moderate COVID-19 have high amounts of SARS-CoV-2 viral RNA in their nasopharynx compared with older children and adults” (29). Taken together, these data imply that, although the viral load in the nasopharynx may be higher in symptomatic children, overall, children remain markedly more resistant to viral infection of the lower respiratory tract leading to COVID-19. All this raises the likelihood that, although children are, fortunately, less susceptible to viral infection of the lungs, they can still serve as good disseminators of the SARS-CoV-2 virus that lurks in their nasal mucosa. Detailed contact tracing from the Korean CDC revealed that household contacts of COVID-19−positive children ages 10 y to 19 y were the most likely to become infected with the SARS-CoV-2 virus compared to household contacts of people of all other ages. In contrast, household contacts of positive children aged 0 y to 9 y were the least likely to become infected. Taken together, these data need further substantiation, and might have implications for spread of infection at home, in daycare, and in schools (30). These data all emphasize that there is much to learn and to consider on the spread from children in various environments. It will also be important to stratify children by age, as infants, young children, and adolescents have different propensities for communicating viral infection.
Immunological Interference.IFNs, first described in 1957 by Isaacs and Lindemann, bind to three distinct types of IFN receptors (31). Mapping of immune response modules in the respiratory tract shows that gene modules triggered by both type 1 and type 2 IFN responses are prominent (17, 18, 32, 33). The type 1 IFN response is vital for viral killing. Type 1 IFN, however, stimulates expression of the ACE2 receptor for the SARS-CoV-2 virus (33). Thus, the virus drives an increase in type 1 IFN expression, which then enhances expression of its receptor in the airway (33). In contrast, coronaviruses that frequently infect children with common colds down-regulate ACE2 as described above (26). Thus, children may benefit from a virtuous cycle with decreased ACE2 leading to less induction of the IFN response, which, in turn, further attenuates ACE2 expression. In contrast, adults suffer from a vicious cycle in which increased ACE2 expression drives a more robust IFN response. The adaptive immune response to common coronavirus infection in children could provide some protection to COVID-19 since they share considerable degrees of homology with coronaviruses associated with the common cold. For example, spike proteins of the common HCoV share 30% amino acid identity with these viruses when one performs Basic Local Alignment Search Tool searches comparing these viruses. A detailed mapping of known T and B cell epitopes on SARS-CoV-2 indicates that adaptive immune reactivity at the T cell and antibody level targets not just the spike region but also other viral proteins (34). A study in adult donors, age currently greater than 20 y, tested whether there was detectable immunity to SARS-CoV-2 and to common cold viruses attributed to coronavirus strains HCoV-OC43, HCoV-HKU1, HCoV-NL63, and HCoV-229E. Donors were recruited between 2015 and 2018, obviating exposure to SARS-CoV-2. Unexposed donors had T cell immunity to both spike and nonspike proteins in SARS-CoV-2 (34). The immunity may have emanated from shared regions on the common cold virus and SARS-CoV-2. Investigators tested immunity to one betacorononavirus HCoV-OC43 and to one alphacoronavirus NL63, and showed that these unexposed donors, n = 11, all had IgG to the receptor-binding domain of these common cold viruses. These nonexposed donors also had vigorous T cell responses to both spike and nonspike proteins in SARS-CoV-2 (35). Additional studies have been reported demonstrating widespread immunity in healthy individuals to cross-reactive regions of SARS-CoV-2 that share peptide sequence homology with endemic coronaviruses that cause common colds like HCoV-OC43, HCoV-229E, HCoV-NL63, and HCoV-HKU1 (36, 37). Humoral, antibody immunity to SARS-CoV-2 is widely detected in individuals, including children, who were not exposed to SARS-CoV-2 (38). Immunity to earlier exposures to both alpha and beta coronaviruses may thus engender protective humoral and cellular immunity for children who are heavily exposed to these common cold viruses. A publication (39) from the Department of Defense examining the effect of the 2017–2018 seasonal influenza vaccine on respiratory infections produced some intriguing results. Investigators showed that the seasonal influenza immunization protected against influenza, as it was intended to do, and protected against some other respiratory viruses. However, they noted a small but statistically significant increase in individuals testing positive to metapneumovirus and coronaviruses. If future influenza vaccines, for example the 2020–2021 seasonal influenza vaccine, also provide increased occurrence of common coronaviruses, this phenomenon may actually afford some protection to SARS-CoV-2. Recent studies show that those with immunity to common coronaviruses do have adaptive immunity to SARS-CoV-2 via the mechanism of cross-reactive immunity (35⇓–37). There is some precedent for this phenomenon. Some immunizations induce protection against other infections outside of the intended target of the vaccine itself (40). A study from the Mayo Clinic indicated that “polio, Hemophilus influenzae type-B (HIB), measles-mumps-rubella (MMR), varicella, pneumococcal conjugate (PCV13), geriatric flu, and hepatitis A/hepatitis B (HepA-HepB) vaccines administered in the past 1, 2, and 5 y are associated with decreased SARS-CoV-2 infection rates” (41). Some antiviral vaccines like the MMR vaccine contain components that have structural similarities with SARS-CoV-2 (42, 43). There is a 29% amino acid sequence homology between the ADP ribose-1-phosphatase domains of SARS-CoV-2 and rubella virus, including surface-exposed conserved residues shared between SARS-CoV-2 and the attenuated rubella virus in MMR (42). Patients with COVID-19 infection had raised levels of rubella IgG, but did not have increased rubella IgM, nor did they have increased levels of antibody to varicella zoster. The investigators interpret these results as indicative of a cross-reactive recall antibody response, common to regions shared between rubella and SARS-CoV-2, that may modulate the course of disease in COVID-19 (42). Whether or not such an immune response is protective or whether such an immune response might potentially enhance disease are outcomes under investigation (42).
|